


Health: foundation or flourishing?
Two straws one cup

Introduction
Two professionals pack their bags before work.
Both say: “I’m off to improve health.”
One packs plasters, painkillers, and antibiotics.
The other packs Frankl’s book, Man’s Search for Meaning, a guide to resilient communities, a therapist’s number, a life coach’s contact, and a quote from a local priest.
They nod on the way out, thinking they’re on the same mission.
They’re not.
One sees health as fixing what’s wrong. The other sees health as helping people live well. For a while, they coexist - quietly, even productively. But when asked to share a budget, draw water from the same well, the realisation hits.
It’s no longer just a health strategy - it’s a prioritisation problem.
In 1920 public “health” meant clean air, safe water, and modest protections so that life was “adequate for the maintenance of health.” Today, it speaks of wellbeing, belonging, connection, even joy – seeing health as wellness and flourishing. But did we ever complete the simpler task we started?
In stretching from health to wellbeing, did we neglect those still left suffering?
From the point of view of the most unwell - those sleeping rough, dying young, or lost in cycles of crisis - would they have been better off if we’d kept the original mission, a focus on fixing all along?
This article explores that trade-off - not to dismiss flourishing, but to ask whether that’s a suitable role and goal for local government, and at what cost. To ask whether we expanded the understanding of “health” too far, too fast, and if it’s time to scale back.
This article is written for anyone who helps shape what ‘health’ means in practice - whether in government, the economy, civil society, or daily life.

At-a-glance
Health has two competing definitions:
One sees health as the absence of illness (relief from suffering).
The other sees health as flourishing (presence of functioning, resilience, purpose, connection, and joy).
Tension arises when these definitions share budgets, responsibilities, or public expectations, particularly within constrained systems like local government or the NHS.
Mission creep. Shifting from “fixing” to “flourishing” risks diluting impact and leaving core needs unmet.
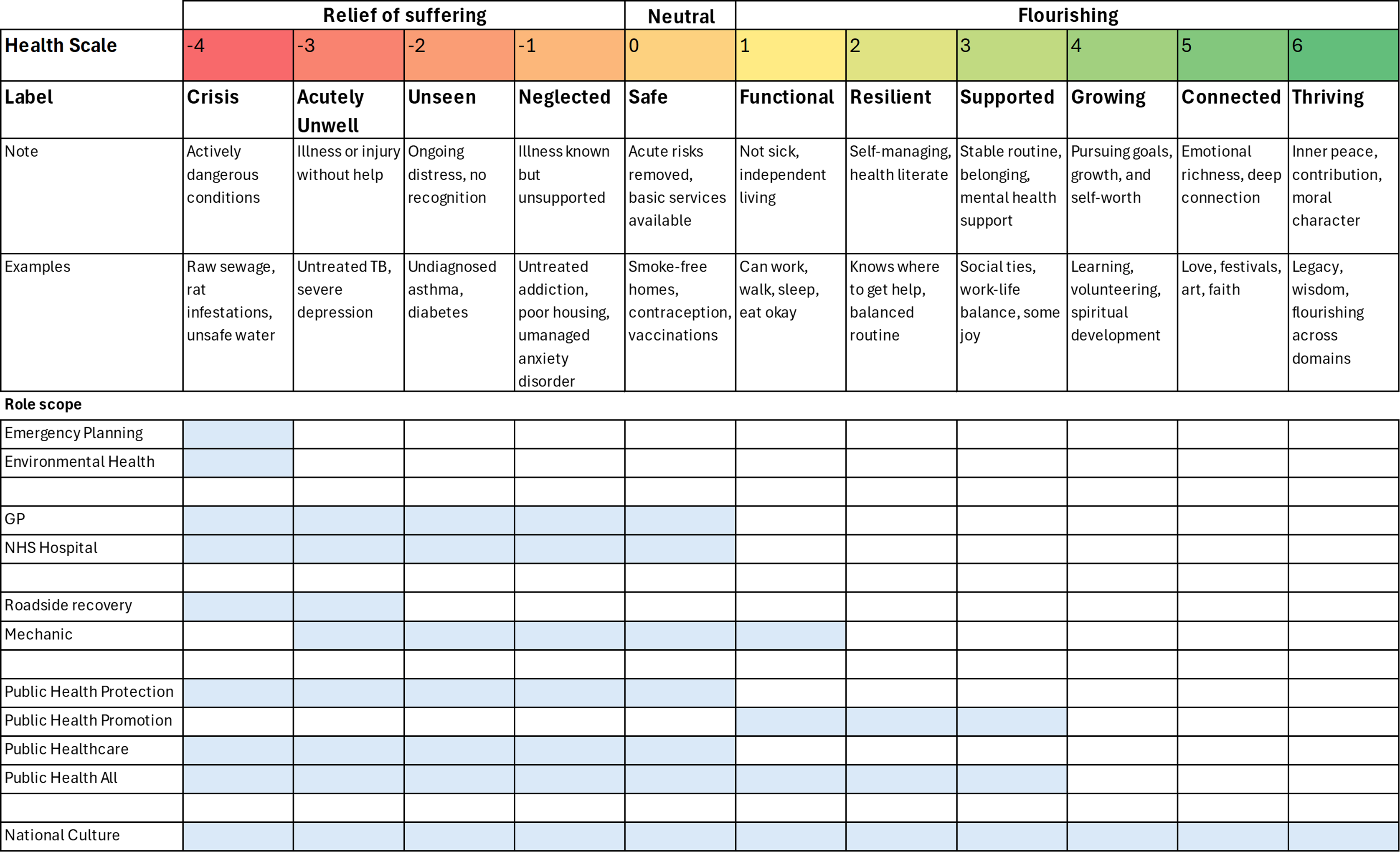
We must reflect on priorities, trade-offs, and the appropriate roles of government, community, and individuals in delivering each part of the health scale (image below).
We need tools (like the health scale) to clarify what kind of health work is being done, and at what cost, to whom, and with what justification.
The two meanings of “Health”
Let’s look at two ends of the spectrum.
1) Negative framing: health as the absence of illness
Health as “not ill.”
Under this understanding the goal of health is to move people from illness to baseline; from deficit to zero; from drowning to floating. That means removing disease, danger, or distress to restore basic functioning.
It focuses on reducing the biggest blocks to health for the masses, and especially those suffering most, and stops there. It gets you to the start line, then leaves the rest up to you and others.
The aim is to keep most people above water - accepting life’s luck and difficulties - and to bounce them back quickly when they dip below it.
Examples in Public Health:
Fix damp housing
Ensure clean air and water
Remove asbestos, lead paint, rats
Control preventable infectious diseases
Reduce second-hand smoke
A fast and effective national health service that functions as a national sickness recovery service (bounce back)
Analogies:
Gardener: Pulls up dangerous weeds, doesn’t plant or prune.
Mechanic: Fixes breakdowns doesn’t service or upgrade.
Doctor: Treats illness, not meaning, financial hardship, stress, or relationships.
Philosophical Grounding:
Arthur Schopenhauer: The goal is to relieve suffering, the only active force. Other desires come and go.
Historical Grounding:
1920 Winslow definition of Public Health: Focuses on sanitation, infection control, hygiene, and basic treatment. Public health as the system that enables “every individual in the community a standard of living adequate for the maintenance of health” (See Definitions).
2) Positive framing: health as wellbeing
Health as wellbeing and flourishing.
Under this understanding health is more than the absence of illness, it’s the presence of wellbeing, purpose, and belonging. Definitions tend to be holistic, expansive, and theoretically limitless. At minimum physical, mental, emotional, and social wellbeing are in the mix. For many spiritual and transcendent aims are top of the tree.
The goal is not just to treat illness, but to create the conditions where people can thrive. It’s proactive, nurturing, and systemic: focused on enabling lives that feel healthy, connected, and meaningful. It performs a remarkably similar role to high culture.
Examples in Public Health:
Mental and emotional wellbeing education in schools
Online parenting classes and support
Community storytelling and arts programmes
Initiatives to reduce loneliness and build social ties
Promotion of the “5 Ways to Wellbeing” framework
Improving subjective wellbeing measures
Analogies:
Gardener: Enriches soil, plants for beauty and resilience, prunes for growth, and shares knowledge. Focused on long-term flourishing, not just weed removal.
Mechanic: Tunes and optimises regularly. Enhances performance, safety, and comfort - not just emergency repairs.
Doctor: Sees the whole person; mind, body, social life, and goals. Partners with patients to support a meaningful, healthy life. May delegate soul to religion or secular alternative.
Philosophical Grounding:
Aristotle: True health is eudaimonia. A life of purpose, virtue, and fulfilment
Historical Grounding:
2025 Faculty of Public Health definition of public health: “The science and art of promoting and protecting health and well-being, preventing ill health and prolonging life through the organised efforts of society.” (See Definitions).
A self-assessment scale
To help visualise this, here’s a scale showing ten stages of health – from negative, to neutral, to positive: representing the different understandings of health and resulting actions in the mix.

With example roles.
Reflection: Where Are You Working?
Having mapped out the terrain, I found myself wondering where I - and the work I’m part of – focus most on this scale. And whether that matches actual need and organisational purpose. The following prompts helped me challenge assumptions, confront trade-offs, and re-imagine what health work could look like. You might find them useful too.
Locate your position
Where does your current work sit on the health scale from crisis (-4) to thriving (+6)?
Are you focused on relieving suffering, maintaining safety, boosting flourishing or something else entirely?
Is that where the need is greatest? Where the impact is highest? Or just where the funding allows?
Consider trade-offs and responsibilities
What if the presenting issues land in suffering but the root causes land in flourishing (stable loving home in formative years)?
What should the limits be on public spending and reach across this scale? Where do you want your taxes to go?
How should roles be divided between government, individuals, families, communities, and the private sector? Is there a bigger role for government on the deficit side or smaller? What about in flourishing?
Is your programme doing what it’s best placed to do, or trying to fill every gap?
Name patterns and asymmetries
Is all the talk about wellbeing, but all the action about survival?
Is “mental health” doing the word work of mental illness, mental health, and mental wellbeing all at once?
Is work on mental health more likely to be stretched across the full scale, from harm to flourishing. than physical health? Why might that be?
Examine your philosophical stance
Is your actual role in health closer to Schopenhauer (relieving suffering) or Aristotle (cultivating virtue)?
What about your own views, outside your professional role?
Do your actions align with your values, or are they more shaped by outside influences?
Make the hard choices
Does more help for those at levels 2–6 mean less help for those in crisis?
What gets overlooked if we focus only on negative health levels (-4 to 0)?
Is focusing on survival morally better than investing in thriving?
Should everyone be assured of survival before a pound goes on flourishing – or should we run both aims in parallel?
What balance …10% foundation 90% flourish? Or 90% foundation 10% flourish?
What gets diluted, or lost, if we try to do everything with a fixed budget?
If you had £100 per person per year, where would you invest it?
Help everyone reach zero first? Move all money allocated to people who are flourishing to those lacking a foundation?
Spread it evenly across the scale? Help all equally.
Prioritise growth for those already stable? People who are stable or thriving tend to want to help others, so more people moved up the scale could mean more relief of suffering via non-governmental routes: private, civic, and economic routes.
Foundations or Flourishing?
Most government public health systems were built in the spirit of Schopenhauer: to relieve suffering. In health terms, that’s work at levels -4 to 0: removing harm, stabilising lives, restoring function.
Increasingly, though, agencies like the NHS and local government are being asked to move further up the scale, towards resilience, connection, wellbeing, purpose, even joy. Sometimes this is intentional. Sometimes it’s quiet role creep.
That shift would be fine if the investment grew with the ambition, like a business scaling based on customer demand, but often, it hasn’t. In fact, the scope has expanded, while real-term resources have shrunk.
Some might argue the health system hasn’t truly invested in flourishing, only adopted its language. And that much of the “wellbeing” talk remains aspirational, not material.
But even aspirational creep has consequences. It shapes how we frame success, write strategies, justify programmes, and distribute attention. It can blur roles, stretch expectations, and pull focus from those in greatest need.
The wider focus carries a hidden trade-off. Less relief of suffering.
We now have two thirsts to quench, two straws drawing from the same milkshake: one for survival, one for taste.
Should they both be in there?
If not, is it time to partially reorient? To trim back and rebuild the basics before reaching higher?
Sometimes more is more: a larger remit results in a larger impact.
Sometimes less is more: a focused remit delivers deeper results.
And sometimes, more is less: stretched too thin to make a difference.
What “more” are we aiming for in health? Was Winslow right one hundred years ago in shooting for “adequate.”
Calls to action
For professionals or decision-makers:
Reflect on where your work currently sits on the health scale.
Ask: Are we meeting the foundational needs before pursuing flourishing?
Use the scale to guide resource allocation, programme design, and role clarity.
Name and confront trade-offs more openly in policy conversations.
For curious or civically engaged readers:
Question what you think health means, and what you expect from your government, your economy, and your local civic or public life.
Think about where your taxes should go on the health scale.
Consider the balance between personal responsibility, civic society, private trading and public provision in creating a flourishing society.
More in this series
This piece is part of a series exploring:
What kind of health thinker are you? 5 Foundational Questions
What kind of health thinker are you? 7 Ticklish Topics
The £3 Billion Question: What Really Counts as Public Health?
Equality before freedom? What do we really value most?
Appendix 1: Definitions
Definition of Public Health (1920, Charles-Edward A. Winslow)
“Public Health is the science and the art of preventing disease, prolonging life, and promoting physical health and efficiency through organised community efforts for the sanitation of the environment, the control of community infections, the education of the individual in principles of personal hygiene, the organisation of medical and nursing services for the early diagnosis and preventive treatment of disease, and the development of the social machinery which will ensure to every individual in the community a standard of living adequate for the maintenance of health.
In its widest sense, Public Health is concerned with the total system which assures the conditions under which people can be healthy.”
Specific basics like a clean environment, infectious disease control, personal hygiene, reasonable detection and treatment of disease, are the means to a modest goal: “adequate for the maintenance of health.”
Contrast this with the 2025 Faculty of Public Health definition of public health as:
“The science and art of promoting and protecting health and well-being, preventing ill health and prolonging life through the organised efforts of society.”
This definition intentionally includes both the scientific (evidence-based, data-driven) and artistic (judgement, collaboration, and communication) elements of public health, and highlights its collective nature. Emphasising that improving health is not just about healthcare, but about well-being and the coordinated efforts across all sectors of society.
Appendix 2: Sources
Brookfield, S. (2023). What isn’t public health? Journal of Public Health Policy, 44(2), 264–275. https://doi.org/10.1057/s41271-023-00404-x
Coggon, J. (2023). What Is Public Health? London: Faculty of Public Health. Aνακτ\acute\etaþetaηκε Στıotaς, 24(04), 2024. https://www.fph.org.uk/media/2afgi1gm/what-is-public-health.pdf
Epstein, R. A. (2003). Let the shoemaker stick to his last: a defence of the ‘old’ public health. Perspectives in Biology and Medicine, 46(3 Suppl), S138-159.
Faden, R., Bernstein, J., & Shebaya, S. (2025). Public Health Ethics. In E. N. Zalta & U. Nodelman (Eds.), The Stanford Encyclopaedia of Philosophy (Spring 2025). Metaphysics Research Lab, Stanford University. https://plato.stanford.edu/archives/spr2025/entries/publichealth-ethics/
Gostin, L. O., & Bloche, M. G. (2003). The politics of public health: a response to Epstein. Perspectives in Biology and Medicine, 46(3 Suppl), S160-175.
Horton, R. (2011). Offline: Where is public health leadership in England? The Lancet, 378(9796), 1060. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(11)60976-8/abstract
Kass, N. E. (2001). An Ethics Framework for Public Health. American Journal of Public Health, 91(11), 1776–1782. https://doi.org/10.2105/AJPH.91.11.1776
McManus, J. (2021). "Human flourishing is a moral and a social, enterprise: a commentary on Mackay." (“Human flourishing is a moral and a social, enterprise: a ... - PubMed”) Journal of Public Health, 43(3), e425–e426. https://doi.org/10.1093/pubmed/fdaa011
What Makes Health Public?: A Critical Evaluation of Moral, Legal, and Political Claims in Public Health (Introduction). (n.d.). Retrieved 24 March 2025, from https://www.southampton.ac.uk/assets/imported/transforms/content-block/UsefulDownloads_Download/13B28FD62773426DAC6AA616448001A6/WMHP%20-%20Intro.pdf
Appendix 3: Fragments of insight related to “Health”
Not all thoughts belong at all moments. A healthy mind can compartmentalise where it needs to, with heavy doors that shut securely.
And so the healthy mind too must be ready for all eventualities.
Healthy negative emotions are generally less profoundly uncomfortable and less problematic than their unhealthy counterparts, for example, feeling intensely sad, a healthy negative emotion, is less uncomfortable than feeling intensely depressed, an unhealthy emotion. Sadness may prompt you to do something to improve the situation (a constructive behaviour), but depression is more likely to leave you to inaction and resignation, an unconstructive behaviour.
Virtue alone is good, vice alone bad. Everything else traditionally assigned a positive or negative value – health or illness, wealth or poverty, sight, or blindness, even life or death – is 'indifferent'.
When millions of individuals are left to determine their own destinies, through trial and error, they tend to make good decisions, and the collective outcome is much better than if a society has been planned from the centre. The free society frequently restores health and vigour to the constitution, in spite not only of the disease, but of the absurd prescriptions of the doctor (government)
On the focus and attention that is part of good mental health. Are thoughts must be arranged, as it were, in little drawers, so that we may open one without disturbing any of the others.
That genuine profound peace of mind, that perfect tranquillity of soul, which next to health, is the highest blessing the earth can give, is to be attained only in solitude. And, as a permanent mood, only in complete retirement; and then, if there is anything great in the man's own self, his way of life is the happiest that may be found in this wretched world.
Happiness is cheerfulness. It rests on health, which rests on exercise. Life is movement. It is its very essence.
What are some of the ways of showing and telling who you are and how you're feeling? They may be sports or homemaking or art or music or crafts or science or maths or dance or selling or public speaking. Whatever they may be, and if you know they are healthy, try to keep embracing them, love them, give them room to grow inside yourself because those gifts of expression are so unique to you.
Those who can appreciate others - who look for what is good, healthy, and kind - are those close to the eternal good. Those who are always looking for what is bad about themselves, or others are really on the side of evil.
In the same way that we understand infant crying as nonverbal communication because they have not learnt language: in adulthood is mental health, neurosis, or psychosis the communication of something unsaid or unfelt or untapped into? Symbolic communication from the unconscious?
Cognitive empathy (perspective taking), emotional empathy (feeling with), compassionate (think, feel and potentially act with healthy detachment)